


Medication Risk-Benefit Calculator
Understand your personalized medication risks and benefits with this evidence-based tool. Based on clinical studies, patients using decision aids improve medication safety by understanding their specific risk reduction and trade-offs.
Your Health Factors
How This Works
Based on the Statin Choice tool used in clinics, this calculator shows:
- How your specific risk changes with medication
- What a 1.1% absolute reduction means in real terms
- How to weigh benefits against side effects
Your Personalized Risk Assessment
What This Means for You
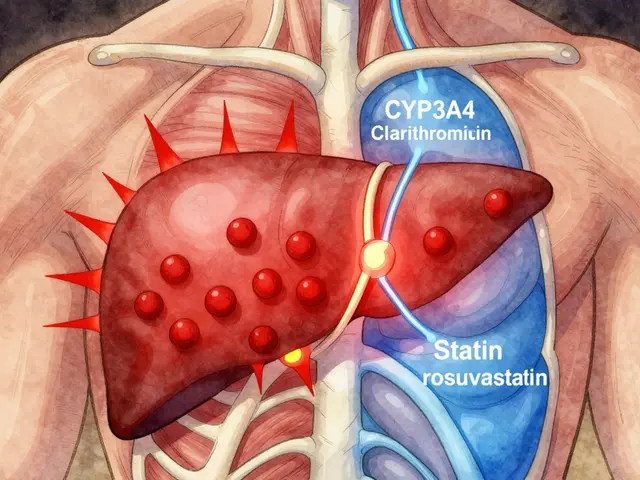
Based on your inputs, taking this medication would reduce your heart attack risk from 7.2% to 6.1%. This represents a 1.1% absolute reduction in risk. You should also consider the 5% chance of experiencing muscle pain.
Every year, hundreds of thousands of people in the U.S. and UK are harmed by medication errors-not because doctors prescribe wrong doses, but because patients don’t fully understand what they’re taking, why, or what the trade-offs are. This isn’t about negligence. It’s about complexity. A statin might lower your risk of a heart attack by 15%, but it also carries a 5% chance of muscle pain. An insulin regimen might control your blood sugar, but it demands strict timing and carries risk of low blood sugar. When patients aren’t clear on these numbers, they either refuse needed meds or take them without knowing the real risks. That’s where patient decision aids come in.
What Are Patient Decision Aids, Really?
Patient decision aids aren’t brochures. They’re not apps that just list side effects. They’re structured tools-paper, digital, or video-that walk you through your options with real data, not vague warnings. They show you: what happens if you take this drug, what happens if you don’t, and how your values fit into the equation. Did you know? Over 150 of these tools are officially validated against the International Patient Decision Aids Standards (IPDAS), meaning they’ve been tested to make sure they’re balanced, clear, and free of bias.Take the Statin Choice aid, used in clinics across the U.S. and Canada. It doesn’t just say, “This lowers your heart attack risk.” It shows you, based on your age, cholesterol, blood pressure, and smoking status, that your 10-year risk is 7.2%. Then it says: if you take this pill, that drops to 6.1%. That’s a 1.1% absolute reduction. Some patients think that’s worth it. Others don’t. The tool doesn’t push one answer. It just helps you decide.
How Do They Actually Improve Medication Safety?
Medication errors happen when people start, stop, or skip drugs because they’re confused. Decision aids cut that risk by making the invisible visible. Here’s what the evidence shows:- Patients who use decision aids score 13.28 points higher on knowledge tests than those who just get a verbal explanation.
- They’re 43% less likely to stay undecided about their treatment-meaning fewer people just avoid making a choice.
- They show more accurate understanding of risk. One study found patients using a diabetes decision aid changed their perception of stroke risk by an average of 38% after using the tool.
- Medication adherence improves by up to 17.3% at six months, especially for chronic conditions like diabetes and high blood pressure.
At the Mayo Clinic, after embedding decision aids into their diabetes care pathway, medication adherence jumped from 58% to 75% in just six months. That’s not magic. That’s clarity.
They’re Not Just for Tech-Savvy People
A common myth is that decision aids only work for educated, tech-literate patients. That’s not true. The most effective ones are designed for low-literacy users. Many include:- Simple icons instead of complex graphs
- Audio narration for those who struggle to read
- Large fonts and high-contrast displays
- Teach-back methods-where the clinician asks, “Can you tell me in your own words what you’re deciding?”
One patient on Reddit, u/Type2Journey, shared how a decision aid changed his life: “My doctor said I was ‘high risk’ for heart disease. The tool showed me my actual risk was 7.2%. I didn’t need a statin. I saved myself from muscle pain and monthly pills.” That’s the power of personalized, data-driven clarity.
What Makes Them Different From Regular Patient Education?
A pamphlet says: “Take your blood pressure medicine daily.” A decision aid says: “Here’s what happens if you take it. Here’s what happens if you don’t. Here’s how your fear of side effects compares to your risk of stroke. What matters most to you?”The key difference is values clarification. Most educational materials focus on facts. Decision aids force you to ask: “Is avoiding a headache worth a 1% higher chance of a stroke?” That’s not something a doctor can guess. Only you know.
Studies show that when patients use decision aids, their involvement in care-measured by the OPTION scale-rises by 22 points compared to standard care. That’s not a small change. That’s a transformation from passive recipient to active partner.
Are They Used in Real Clinics?
Yes-and adoption is growing fast. In 2015, only 12% of U.S. primary care doctors used them. By 2022, that jumped to 37%. Why? Because the system is changing.- Medicare Advantage plans now reward doctors for using shared decision-making tools.
- 29 U.S. states have passed laws requiring decision aids for certain procedures and medications.
- 68 of the top 100 U.S. health systems now use them in at least one specialty-especially in cardiology, oncology, and endocrinology.
Tools like the Ottawa Hospital Research Institute’s Decision Aids Library offer over 100 free, validated tools that clinics can download and use. Many integrate directly into electronic health records through FHIR APIs, so the clinician doesn’t have to switch screens. One clinic in Leeds reported cutting decision-making time by 30% after switching from paper to digital aids that auto-populated patient data.
What’s the Catch?
Nothing’s perfect. Decision aids have limits.- They add 3 to 8 minutes to a visit. In a 15-minute slot, that’s hard to fit. The fix? Give patients the tool to review at home before the appointment.
- Some elderly or cognitively impaired patients feel overwhelmed. That’s why simplified versions and caregiver support are critical.
- Not all tools are created equal. Only IPDAS-certified tools have been proven to work. Many apps and websites claim to be decision aids but just dump info without helping you weigh values.
- Reimbursement is still patchy. If a doctor’s paid per visit, not per outcome, they may skip the extra time-even if it saves money long-term.
And yes, there’s still debate. Some researchers, like Dr. Michael Barry from JAMA, point out: we don’t yet have strong proof that decision aids reduce hospitalizations or deaths. But we do know they reduce confusion, reduce unnecessary prescriptions, and increase trust. That’s a win for safety.

How to Get Started-For Patients and Clinicians
If you’re a patient: Ask your doctor, “Do you use any tools to help patients decide about medications?” If they say no, suggest the Ottawa Decision Aid Library. It’s free, evidence-based, and available in multiple languages.If you’re a clinician: Start with one condition-maybe statins or diabetes meds. Pick one IPDAS-certified tool. Try it with three patients. Track what changes: Do they ask better questions? Do they stick to the plan? You’ll see the difference.
Training takes just 2-3 hours. The IPDAS Collaboration offers free webinars, and Slack communities with over 1,800 clinicians sharing tips. You don’t need to be a tech expert. You just need to be willing to let patients lead the decision.
The Future Is Personalized
The next wave of decision aids is AI-driven. The NIH is testing a system that pulls your EHR data-meds, lab results, genetics-and builds a custom risk profile in real time. Imagine walking in for your blood pressure check, and your doctor says, “Based on your kidney function and your fear of dizziness, here’s what your options look like.” That’s not science fiction. It’s coming by 2027.The FDA already recognizes certain decision aids as part of medication labeling for complex drugs. CMS plans to expand requirements to 12 more clinical areas by 2025. The message is clear: if a decision involves trade-offs, and patient values matter, then a decision aid belongs in the room.
Medication safety isn’t about better pills. It’s about better decisions. And decision aids are the simplest, most proven tool we have to make sure those decisions are truly yours.
Do patient decision aids really reduce medication errors?
Yes. Studies show they reduce errors by improving patient understanding of risks and benefits. Patients who use validated decision aids are less likely to start unnecessary medications, stop needed ones, or misunderstand dosing instructions. One study found a 38% improvement in risk perception accuracy after using a decision aid for diabetes meds.
Are patient decision aids only for chronic conditions?
No. While they’re most common for chronic diseases like diabetes, high blood pressure, and statin therapy, they’re also used for antibiotics, pain meds, mental health drugs, and even short-term treatments like anticoagulants after surgery. Any time there’s more than one reasonable option-and patient values matter-they’re helpful.
Can I use a patient decision aid on my own, without a doctor?
You can use them to prepare, but they’re not meant to replace clinical advice. Decision aids help you understand options and clarify your values so you can have a better conversation with your provider. They’re a tool for shared decision-making, not self-diagnosis. Always discuss your choices with a clinician before making changes to your treatment.
Are patient decision aids free to use?
Many high-quality, evidence-based decision aids are free. The Ottawa Hospital Research Institute’s library offers over 100 validated tools at no cost. Some commercial platforms charge for advanced features or EHR integration, but the core tools used in clinics are typically funded by public health systems or research grants.
How do I know if a decision aid is trustworthy?
Look for the IPDAS certification logo or mention of the International Patient Decision Aids Standards. Trusted sources include the Ottawa Hospital Research Institute, the National Institutes of Health (NIH), and the Agency for Healthcare Research and Quality (AHRQ). Avoid tools that push one option, lack data sources, or don’t include values clarification exercises.
What Comes Next?
If you’re a patient, the next step is simple: ask. If you’re a clinician, pick one decision aid and try it with your next patient. Track the outcome. You might be surprised by how much clarity changes behavior.The goal isn’t to make every patient an expert. It’s to make sure every patient’s choice is theirs-based on real information, not fear, pressure, or confusion. That’s the heart of medication safety. And patient decision aids are the quiet revolution making it happen.














nithin Kuntumadugu
12 Dec 2025 at 04:40lol so now we're giving patients *decision aids*? next they'll hand out flowcharts for when to cry during commercials. this is just the medical-industrial complex trying to offload responsibility. i bet the statin makers paid for this 'tool'. 🤡