


Living with cirrhosis is a serious condition that demands constant vigilance. The biggest threat isn't just the scarring of your liver; it's the silent development of hepatocellular carcinoma (HCC), the most common type of primary liver cancer. In fact, over 80% of all HCC cases occur in people who already have advanced fibrosis or cirrhosis. This makes cirrhosis the single most significant risk factor for developing this disease. The good news? Early detection changes everything. When caught early, HCC is treatable, often curable, and survival rates jump dramatically-from roughly 10-20% in unscreened populations to 50-70% in those under active surveillance.
You might wonder why we don’t screen everyone. It’s because not every person with liver damage is at equal risk. Guidelines from major organizations like the American Association for the Study of Liver Diseases (AASLD) and the European Association for the Study of the Liver (EASL) have evolved to help doctors target resources where they matter most. Understanding these protocols isn't just academic-it’s about saving lives by catching tumors before they grow too large or spread.
Who Needs HCC Surveillance?
The core rule is simple: if you have cirrhosis, you need regular monitoring. But not all cirrhosis is the same. Doctors use the Child-Turcotte-Pugh (CTP) score to classify how well your liver is functioning. Patients with CTP Class A or B cirrhosis are strong candidates for standard surveillance. These patients generally have preserved enough liver function to benefit from potential treatments if cancer is found.
However, the approach shifts for those with CTP Class C cirrhosis. The AASLD strongly recommends against routine surveillance for this group unless they are on a transplant waiting list. Why? Because their median survival without a transplant is less than two years, and aggressive cancer treatments may cause more harm than good. On the other hand, the Asian Pacific Association for the Study of the Liver (APASL) suggests that some select Class C patients with preserved liver function might still benefit from monitoring. This divergence highlights why personalized medical advice is crucial-you aren't just a statistic; your specific health profile dictates your path.
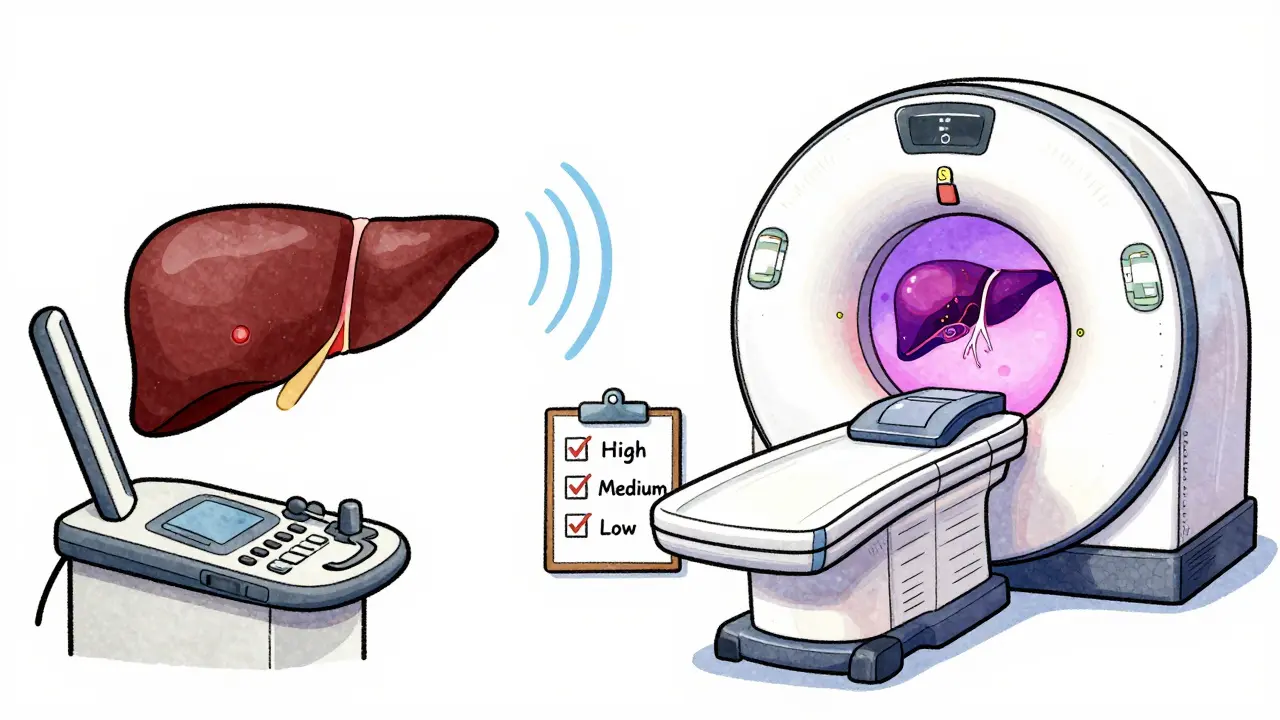
A newer, smarter approach comes from the EASL 2023 Policy Statement. Instead of a "one-size-fits-all" model, they propose risk-stratified surveillance. This method categorizes patients into three tiers based on their annual risk of developing HCC:
- High-risk (>2.5% annual risk): Requires intensive monitoring, potentially using MRI instead of ultrasound.
- Medium-risk (1.5-2.5% annual risk): Standard 6-month ultrasound surveillance.
- Low-risk (<1.5% annual risk): Surveillance might be forgone to reduce unnecessary costs and anxiety.
This stratification could reduce unnecessary tests by 20-30%, focusing energy on those most likely to develop cancer. Tools like the aMAP score (which looks at age, gender, albumin, bilirubin, and platelets) help calculate this risk with high accuracy.
The Surveillance Protocol: Ultrasound and AFP
If you are cleared for surveillance, what does it actually involve? The gold standard remains biannual abdominal ultrasound. You get an ultrasound every six months. This interval isn't arbitrary; studies show that HCC tumors typically grow by 1-2 cm every six months in cirrhotic livers. Catching them within this window keeps them small and manageable.
Many guidelines also recommend adding an alpha-fetoprotein (AFP) blood test. AFP is a protein produced by the liver during fetal development. In adults, high levels can signal liver cancer. The AASLD conditionally recommends checking AFP alongside ultrasounds. If your AFP level exceeds 20 ng/mL, it triggers further investigation. However, keep in mind that AFP isn't perfect-it can be elevated due to active hepatitis or liver regeneration, leading to false alarms. That’s why imaging is always the final judge.
| Guideline Body | Primary Imaging Modality | Frequency | AFP Recommendation | Risk Stratification |
|---|---|---|---|---|
| AASLD (2018) | Ultrasound | Every 6 months | Conditional (if >20 ng/mL) | No (Universal for CTP A/B) |
| EASL (2023) | Ultrasound or MRI | Every 6 months | Optional | Yes (Risk-based tiers) |
| ACG (2020) | Ultrasound | Every 6 months | Recommended | No |
When Screening Comes Back Positive
What happens if your ultrasound shows a suspicious mass larger than 1 cm, or your AFP is high? Don't panic yet. A positive screen doesn't mean you have cancer; it means you need a closer look. All major guidelines mandate immediate follow-up with multiphase contrast imaging, specifically a CT scan or an MRI with liver-specific contrast agents.
These advanced scans are powerful. They have sensitivity rates of 80-90% for characterizing lesions. Doctors use systems like LI-RADS (Liver Imaging Reporting and Data System) to standardize how they describe what they see. LI-RADS helps radiologists communicate clearly with hepatologists, reducing confusion and ensuring you get the right diagnosis faster. If the imaging confirms HCC, the next step is staging to determine treatment options.
Treatment Options for Hepatocellular Carcinoma
Once HCC is diagnosed, treatment depends heavily on two factors: the stage of the cancer and the function of your remaining liver. This is often determined using the Barcelona Clinic Liver Cancer (BCLC) staging system. Here’s a breakdown of the main treatments available today:
- Liver Transplantation: For eligible patients with early-stage HCC and poor liver function, transplantation offers both a cure for the cancer and a solution for the underlying cirrhosis. It’s the ideal option but limited by organ availability.
- Surgical Resection: If your liver function is still good (usually CTP A) and the tumor is confined to one part of the liver, surgeons can remove the cancerous section. This preserves your natural liver.
- Ablation Therapy: For small tumors (under 3-5 cm), doctors can destroy the cancer cells using heat (radiofrequency ablation) or cold (cryoablation). This is minimally invasive and highly effective for early-stage disease.
- Transarterial Chemoembolization (TACE): For intermediate-stage cancers that haven't spread outside the liver, TACE blocks the blood supply to the tumor while delivering chemotherapy directly to it. It starves the cancer of nutrients.
- Systemic Therapies: For advanced stages where local treatments aren't possible, drugs like atezolizumab plus bevacizumab or tyrosine kinase inhibitors (e.g., lenvatinib, sorafenib) are used. These work throughout the body to slow cancer growth.
The goal is always to choose the least invasive option that effectively controls the disease while maintaining your quality of life. Multidisciplinary teams-including hepatologists, oncologists, surgeons, and radiologists-work together to pick the best strategy for your specific case.
Challenges in Implementation
Even with clear guidelines, getting consistent care is hard. Studies show that only 30-50% of eligible patients in the U.S. receive guideline-concordant surveillance. Why? Barriers include lack of provider awareness, no automated reminders in electronic health records, and patient non-compliance. Many patients miss appointments due to fear, discomfort, or simply forgetting. Additionally, disparities exist: White patients are screened at higher rates (52.3%) compared to Black patients (34.1%), and privately insured individuals are monitored more often than those on Medicaid.
To improve this, clinics are adopting better tools. Electronic health record alerts now trigger when a cirrhosis code is entered. Patient navigators help coordinate care, reducing no-show rates from 32% to 14%. As AI-assisted ultrasound tools gain FDA clearance, we may see even better detection rates in the future, making surveillance easier and more accurate for everyone involved.
How often should I get an ultrasound for HCC surveillance?
You should undergo an abdominal ultrasound every six months. This biannual schedule is recommended by major guidelines like AASLD and EASL because HCC tumors typically grow slowly, allowing for early detection within this timeframe.
Is alpha-fetoprotein (AFP) testing necessary?
AFP testing is conditionally recommended by AASLD and optional by EASL. It serves as a supplementary tool to ultrasound. An AFP level above 20 ng/mL warrants further investigation with CT or MRI, though it can sometimes yield false positives due to other liver conditions.
Can HCC be cured if detected early?
Yes, early detection significantly improves outcomes. Curative treatments such as liver transplantation, surgical resection, or ablation therapy offer high success rates when the cancer is caught at Stage 0 or A, boosting 5-year survival rates to 50-70%.
Who is excluded from HCC surveillance?
Patients with Child-Turcotte-Pugh Class C cirrhosis are generally excluded from routine surveillance unless they are candidates for liver transplantation. Their prognosis is often too poor to benefit from aggressive cancer treatments, and the focus shifts to palliative care or transplant evaluation.
What is risk-stratified surveillance?
Risk-stratified surveillance tailors monitoring intensity based on individual risk levels. High-risk patients may receive MRI scans, medium-risk patients get standard ultrasounds, and low-risk patients might skip surveillance entirely. This approach optimizes resource use and reduces unnecessary procedures.



Write a comment