


Shortness of breath is a frustrating symptom. You might feel it climbing stairs or just walking across the room. But what you feel doesn't always match what's happening inside your lungs. That’s why doctors order Pulmonary Function Tests, often called PFTs. These are not just simple breathing exercises; they are precise diagnostic tools that measure how well your lungs move air in and out and how efficiently they transfer oxygen into your blood. The two most critical parts of this evaluation are spirometry and the diffusing capacity of the lung for carbon monoxide (DLCO). Understanding these results can be tricky because numbers alone don’t tell the whole story. A low number isn’t always bad news, and a normal result doesn’t always mean everything is fine. This guide breaks down exactly what these metrics mean, how they work together, and what specific patterns reveal about your respiratory health.
The Basics: What Spirometry Actually Measures
Spirometry is the cornerstone of lung testing. It’s the first step in almost every pulmonary evaluation. When you sit in the clinic, blow hard into a tube, and repeat it three times, you’re generating data that helps doctors categorize your lung disease. The machine measures volume and speed. There are three key numbers you need to know:
- Forced Vital Capacity (FVC): This is the total amount of air you can forcibly blow out after taking the deepest breath possible. Think of it as your lung’s total tank size during exhalation.
- Forced Expiratory Volume in 1 second (FEV1): This is how much of that air you can blast out in just the first second. It measures the speed of your airflow.
- The FEV1/FVC Ratio: This is the most important metric. It compares the speed to the total volume. In healthy adults, this ratio is usually above 0.70 (or 70%). If it drops below that threshold, it signals an obstruction.
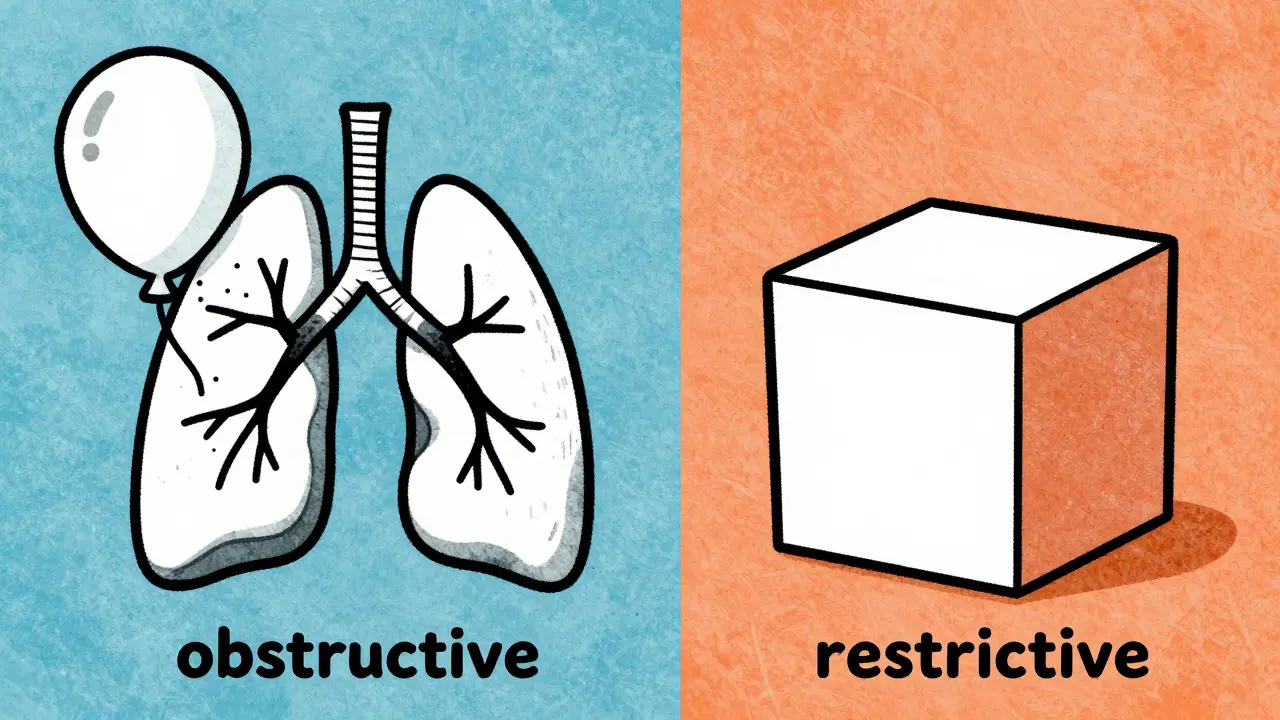
Obstructive vs. Restrictive Patterns
Once you have the spirometry numbers, the next job is to figure out what kind of problem exists. There are two main categories: obstructive and restrictive. Obstructive Lung Disease This pattern means air has trouble getting out. The airways are narrowed or collapsed. You’ll see a reduced FEV1/FVC ratio (less than 0.70). Common causes include asthma, chronic obstructive pulmonary disease (COPD), and emphysema. In these conditions, the FVC might be normal or slightly low, but the FEV1 is significantly lower because the airway resistance slows down the exhalation. Restrictive Lung Disease Here, the lungs can’t expand fully. The airways are open, but the lung tissue or chest wall is stiff or weak. You’ll see a normal or even high FEV1/FVC ratio, but both the FEV1 and FVC are low. The "tank" is smaller than it should be. Causes include pulmonary fibrosis (scarring), obesity, or skeletal issues like kyphoscoliosis.
However, spirometry has a blind spot. It cannot easily distinguish between true restriction (small lungs) and "pseudorestriction." Pseudorestriction happens in severe obstruction when air gets trapped in the lungs, making the FVC look low even though the lungs aren’t actually small. This is where the DLCO test becomes essential.
Understanding the DLCO Test
If spirometry tells you about airflow, DLCO (Diffusing Capacity of the Lung for Carbon Monoxide) tells you about gas exchange. It measures how well oxygen moves from the air sacs (alveoli) into your bloodstream. Why carbon monoxide? Because it binds to hemoglobin so strongly that nearly all of it is absorbed in one pass. This makes it a perfect tracer for measuring the efficiency of the alveolar-capillary membrane. During the test, you take a deep breath of a mixture containing helium, carbon monoxide, and oxygen, hold it for 10 seconds, and then exhale. The machine calculates how much CO was absorbed. The result is expressed as a percentage of the predicted value for someone with your demographics.
- Normal Range: Typically 75% to 140% of predicted.
- Low DLCO: Below 75%. This suggests damage to the lung tissue or blood vessels.
- High DLCO: Above 140%. This is less common but indicates increased blood volume in the lungs or other factors.
Putting It Together: The Diagnostic Algorithm
The real power of PFTs comes when you combine spirometry and DLCO. Doctors use a stepwise approach to narrow down the diagnosis. Here is how different combinations point to specific conditions.
| Spirometry Pattern | DLCO Result | Likely Diagnosis |
|---|---|---|
| Obstructive (Low FEV1/FVC) | Low | Emphysema, Cystic Fibrosis, Early Silicosis |
| Obstructive (Low FEV1/FVC) | Normal/High | Asthma, Chronic Bronchitis |
| Restrictive (Low FVC, Normal Ratio) | Low | Interstitial Lung Disease (ILD), Pulmonary Fibrosis |
| Restrictive (Low FVC, Normal Ratio) | Normal | Extraparenchymal Restriction (Obesity, Chest Wall Deformity, Neuromuscular Disease) |
| Normal Spirometry | Low | Pulmonary Hypertension, Chronic Pulmonary Embolism, Early ILD |
| Normal Spirometry | High | Asthma (during attack), Polycythemia, Pulmonary Hemorrhage |
Why DLCO Is Crucial for Specific Conditions
Let’s look closer at why this distinction matters.
Emphysema vs. Chronic Bronchitis
Both fall under COPD. Both show obstructive patterns on spirometry. But in emphysema, the air sacs are destroyed, reducing the surface area for gas exchange. So, DLCO is low. In chronic bronchitis, the airways are inflamed, but the air sacs are intact. So, DLCO is usually normal. This difference helps doctors tailor treatment.
Pulmonary Fibrosis
In interstitial lung disease, scar tissue thickens the barrier between air and blood. Oxygen struggles to cross it. DLCO drops significantly-often much earlier than spirometry changes. In fact, DLCO can decrease to 60-70% of predicted before any airflow limitation appears, giving a diagnostic advantage of 12-18 months. A DLCO below 35% of predicted is also a strong predictor of poorer survival outcomes.
Pulmonary Hypertension
This is high blood pressure in the lungs. Spirometry is often completely normal. However, DLCO is frequently low because the blood vessels are damaged or remodeled. A specific clue is the FVC/DLCO ratio. If this ratio is greater than 1.6, it strongly suggests pulmonary hypertension, even if other tests are inconclusive.
Factors That Can Skew Your Results
Your PFT results aren’t just about your lungs. Several external factors can make the numbers look worse or better than they really are. Being aware of these helps avoid misdiagnosis.
- Hemoglobin Levels: DLCO depends on hemoglobin to carry the carbon monoxide. If you are anemic (low hemoglobin), your DLCO will appear falsely low. For every 1 g/dL drop in hemoglobin, DLCO decreases by about 1%. Doctors must correct for this using baseline blood tests.
- Smoking: Smoking increases carboxyhemoglobin in your blood, which blocks the binding sites for the test gas. This can falsely lower DLCO by 5-10%. Patients are usually asked to wait several hours after smoking before testing.
- Effort: Spirometry requires maximum effort. If you don’t blow hard enough, the FEV1 will be low, mimicking obstruction. Technicians check for reproducibility-if your best attempts vary too much, the test is invalid.
- Breath-Hold Time: For DLCO, you must hold your breath for exactly 10 seconds. Holding it longer increases absorption (falsely high DLCO); holding it shorter decreases it (falsely low).
When Are These Tests Ordered?
You might wonder why your doctor ordered these specific tests. Common scenarios include:
- Unexplained Dyspnea: Shortness of breath without an obvious cause like heart failure.
- Chronic Cough: Especially in smokers or those exposed to dust/fumes.
- Preoperative Assessment: Before lung surgery, doctors need to know how much reserve you have.
- Monitoring Disease Progression: For patients with known COPD or fibrosis, tracking FEV1 and DLCO over time shows if the disease is stable or worsening.
- Occupational Exposure: Workers in mining, construction, or chemical industries may get screened for early signs of lung damage.
Next Steps After Your Test
If your results are abnormal, don’t panic. PFTs are screening and diagnostic tools, not final verdicts. They guide the next steps. If spirometry shows obstruction, your doctor might try a bronchodilator (like albuterol) and repeat the test. If your FEV1 improves by more than 12%, it suggests reversible airflow limitation, typical of asthma. If DLCO is low but spirometry is normal, your doctor might order a CT scan to look for early fibrosis or a ventilation/perfusion (V/Q) scan to rule out clots. Keep a copy of your results. Compare them year over year. Trends matter more than single data points. A slow decline in FEV1 or DLCO can signal progression long before symptoms worsen.
What is a normal FEV1/FVC ratio?
A normal FEV1/FVC ratio is typically 0.70 (70%) or higher in adults. Values below 0.70 suggest obstructive lung disease, such as asthma or COPD. However, reference ranges can vary slightly based on age and ethnicity, so doctors always compare your result to predicted values for your specific demographic.
Can DLCO be normal in someone with lung disease?
Yes. In conditions like chronic bronchitis or pure asthma, the air sacs remain intact, so gas exchange is efficient, resulting in a normal DLCO. Additionally, early-stage lung diseases might not yet affect diffusion capacity. A normal DLCO does not rule out all lung problems, but it helps narrow the differential diagnosis.
How does anemia affect DLCO results?
Anemia lowers DLCO results because there is less hemoglobin available to bind with the carbon monoxide used in the test. For every 1 g/dL decrease in hemoglobin, DLCO drops by approximately 1%. Doctors correct for this by adjusting the result based on your blood count, ensuring the reading reflects lung health rather than blood levels.
What does a high DLCO mean?
A high DLCO (above 140% of predicted) is uncommon but can occur in conditions that increase blood volume in the lungs, such as polycythemia (high red blood cell count), left-to-right heart shunts, or pulmonary hemorrhage (bleeding in the lungs). It can also be seen in asthma during an acute attack due to increased pulmonary blood flow.
Do I need to stop smoking before a PFT?
Yes, you should avoid smoking for at least 12 hours before the test. Smoking raises carboxyhemoglobin levels in your blood, which competes with the test gas and can falsely lower your DLCO result. It can also irritate your airways, affecting spirometry accuracy. Follow your technician’s instructions carefully for the most reliable results.
How often should I repeat pulmonary function tests?
Frequency depends on your condition. For stable COPD or asthma, tests might be repeated every 1-2 years or when symptoms change. For progressive diseases like pulmonary fibrosis, monitoring may happen every 6 months to track decline. Always follow your pulmonologist’s recommendation based on your specific diagnosis and treatment plan.







Write a comment