


Diabetes Emergency Response Simulator
Scenario A: Severe Hypoglycemia
A person with diabetes becomes confused, sweaty, and unresponsive. Their blood glucose reads 38 mg/dL.
Low Blood Sugar CrisisScenario B: Severe Hyperglycemia
A person is vomiting, breathing rapidly, and has fruity-smelling breath. Blood glucose is 450 mg/dL with positive ketones.
High Blood Sugar CrisisImagine you are with someone who has diabetes. Suddenly, they become confused, sweaty, and unresponsive. Or perhaps they are vomiting, breathing rapidly, and complaining of a stomach ache. These aren't just bad days; they are medical emergencies. Severe hypoglycemia and hyperglycemia are life-threatening conditions caused by diabetes medications interacting poorly with food, exercise, or illness. One involves blood sugar dropping dangerously low; the other sees it skyrocketing to toxic levels. Knowing the difference saves lives.
The stakes are high. According to the American Diabetes Association (2023), severe hypoglycemia is defined as a blood glucose level below 54 mg/dL (3.0 mmol/L) where the person cannot treat themselves. On the flip side, severe hyperglycemia can lead to diabetic ketoacidosis (DKA) or hyperosmolar hyperglycemic state (HHS), both of which carry significant mortality risks if ignored. This guide breaks down exactly what to do in these crises, how to use emergency medications correctly, and why preparation matters more than reaction.
Recognizing Severe Hypoglycemia: The Silent Killer
Hypoglycemia happens when blood sugar drops too low. For most people on insulin or certain oral medications like sulfonylureas, this is the most common acute risk. The brain runs on glucose. When supply cuts off, neurological function fails fast. You might see shaking, sweating, irritability, or slurred speech. In severe cases, the person may seize or lose consciousness entirely.
Here is the critical rule: if the person is conscious and can swallow, give them fast-acting carbohydrates. Use the "Rule of 15." Give 15 grams of carbs-like four glucose tablets or four ounces of regular soda. Wait 15 minutes. Check again. If still under 70 mg/dL, repeat. Do not overfeed them, as this causes rebound hyperglycemia.
But what if they are unconscious? Never pour liquid into their mouth. They will choke. Instead, you need glucagon. Glucagon is a hormone that signals the liver to release stored glucose. It works within minutes. The challenge has always been getting it into the patient quickly. Traditional kits required mixing powder and liquid, a process that terrified many caregivers during a crisis. Newer options have changed the game.
Emergency Treatment for Low Blood Sugar: Glucagon Options
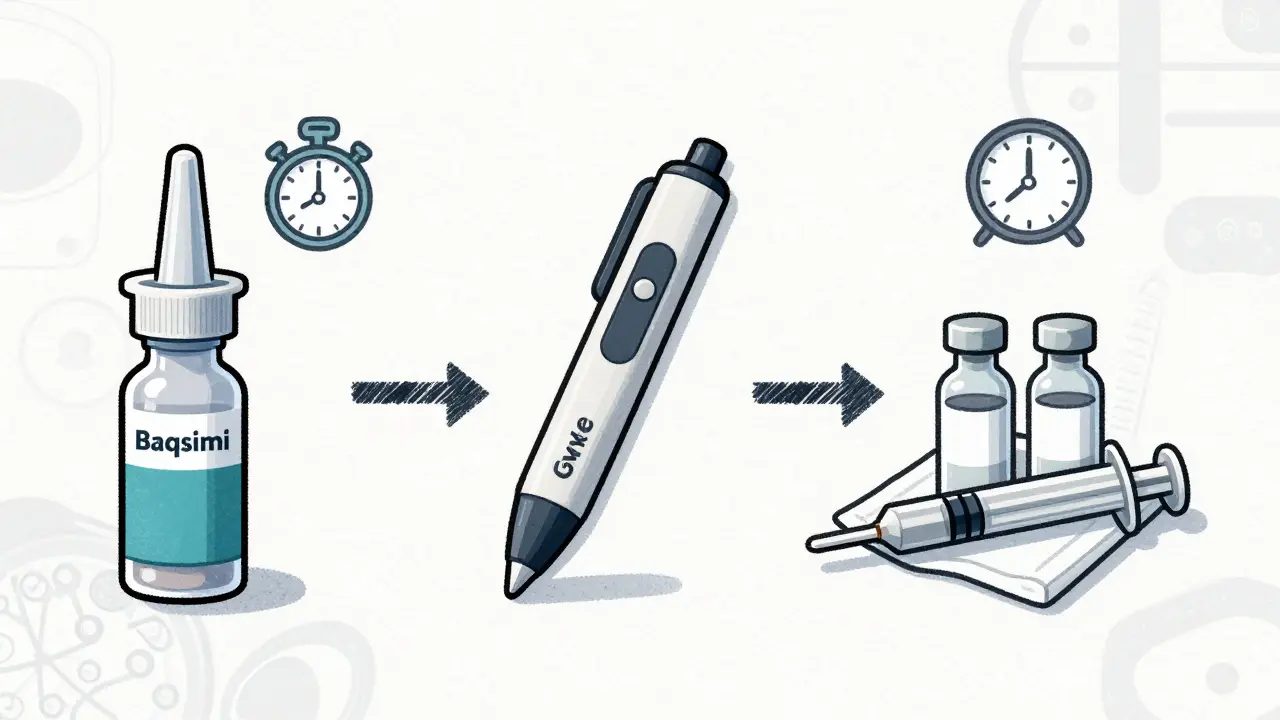
If the person cannot eat or drink, administer glucagon immediately. There are three main types available today:
- Nasal Powder (Baqsimi): Approved by the FDA in 2019, this is often the easiest option. You insert the nozzle into one nostril and press the plunger. No needles, no mixing. Studies show it raises blood sugar effectively within 10-15 minutes.
- Autoinjector (Gvoke HypoPen): This device delivers a subcutaneous injection automatically. You place it against the thigh, abdomen, or upper arm and push the button. It injects 1 mg of glucagon in seconds.
- Traditional Kit: Requires reconstituting powder with saline solution before injecting. While cheaper, it has a higher failure rate due to user error during stress.
A 2021 study published in NASN School Nurse found that 83% of caregivers successfully administered nasal glucagon compared to only 42% with traditional kits. Time is tissue here. Every minute counts. After administering glucagon, turn the person onto their side to prevent aspiration if they vomit. Call emergency services immediately, even if they wake up. Their blood sugar could crash again once the glucagon wears off.
| Feature | Nasal Powder (Baqsimi) | Autoinjector (Gvoke) | Traditional Kit |
|---|---|---|---|
| Administration Method | Intranasal spray | Subcutaneous injection | IM/SubQ injection (mixed) |
| Preparation Time | Seconds | Seconds | 1-2 minutes |
| User Success Rate | 83% | High | 42% |
| Approximate Cost (US) | $268 per unit | $259 per unit | $130 per kit |
Identifying Severe Hyperglycemia: DKA and HHS
Hyperglycemia is the opposite problem. Blood sugar rises above safe limits, often exceeding 250 mg/dL (13.9 mmol/L). In Type 1 diabetes, this frequently leads to Diabetic Ketoacidosis (DKA). When the body lacks insulin, it burns fat for energy, producing acidic ketones. These ketones build up in the blood, turning it acidic. This is a medical emergency.
Symptoms of DKA include frequent urination, extreme thirst, nausea, vomiting, abdominal pain, and fruity-smelling breath. Breathing becomes deep and rapid as the body tries to blow off excess acid. In Type 2 diabetes, patients may develop Hyperosmolar Hyperglycemic State (HHS), where blood sugar skyrockets above 600 mg/dL without significant ketones. HHS causes severe dehydration and confusion.
Do not try to treat DKA or HHS at home. These conditions require hospital care. However, early detection prevents progression. If blood sugar stays above 250 mg/dL despite correction doses, check for ketones. Use urine strips or a blood ketone meter. A blood ketone level above 1.5 mmol/L means you need to go to the emergency department now. Waiting increases the risk of coma or death.
Hospital Protocols for Hyperglycemic Crises
When you arrive at the hospital, doctors follow a strict protocol. The goal is to lower blood sugar slowly while correcting dehydration and electrolyte imbalances. Rapid drops in blood sugar can cause cerebral edema, especially in children.
The standard treatment involves three pillars:
- Intravenous Fluids: Patients receive 1-2 liters of normal saline in the first hour to restore volume. Dehydration is severe in these states.
- Insulin Therapy: Continuous IV insulin infusion starts after fluids begin. A bolus dose may be given initially. Insulin stops ketone production and lowers blood glucose.
- Electrolyte Replacement: Potassium levels drop dangerously during treatment. Doctors monitor potassium closely and add potassium chloride to IV fluids if levels fall below 5.2 mEq/L. Ignoring this can cause fatal heart arrhythmias.
Mortality rates highlight the urgency. Untreated DKA has a 70% mortality rate. With proper treatment, it drops to 1-5%. Never confuse the treatments. Giving insulin to someone with hypoglycemia kills them. Giving glucagon to someone with hyperglycemia makes it worse. Always check blood sugar before acting if possible.
Preparation and Prevention Strategies
Emergencies happen because we are unprepared. Dr. Nitil Kedia’s analysis showed that 73% of severe hypoglycemia episodes occur at home, yet only 28% of at-risk patients received adequate glucagon education. You must bridge this gap.
Create an emergency kit. Include glucose tablets, fast-acting juice boxes, your chosen glucagon formulation, and written instructions. Label everything clearly. Teach family members, friends, and coworkers how to use the glucagon. Practice quarterly. Skills fade without repetition. A 2021 study found that caregivers who practiced retained 92% of skills after six months, compared to 45% who did not.
For hyperglycemia prevention, understand your triggers. Illness, stress, and missed insulin doses are common culprits. Have a "sick day" plan. Test blood sugar and ketones every few hours when sick. Keep hydrated. Never stop insulin unless directed by a doctor, even if you are not eating well. Your body still needs basal insulin to prevent DKA.
Barriers to Access and Equity Issues
Access to emergency care varies widely. Ready-to-use glucagon formulations cost significantly more than traditional kits. Insurance coverage differs. A 2022 ADA report noted that 31% of Medicaid patients faced prior authorization hurdles for glucagon, compared to 12% with private insurance. This delay can be fatal.
Racial disparities also exist. Black and Hispanic diabetes patients experience 2.3 times more severe hypoglycemia-related hospitalizations than White patients. Systemic barriers to education and medication access contribute to this gap. Advocacy groups work to change policies, but individuals must advocate for themselves. Ask your doctor about assistance programs for expensive medications. Know your rights regarding emergency supplies at school or work.
Future Technologies and Hope
Technology is evolving to reduce these risks. Continuous glucose monitors (CGMs) like the Dexcom G7 provide real-time alerts. The Beta Bionics iLet system, approved in 2023, acts as an artificial pancreas, automatically delivering microdoses of glucagon when low blood sugar is predicted. Early trials show a 72% reduction in severe events. While access remains limited, these tools represent the future of diabetes management.
Until universal adoption occurs, knowledge is your best defense. Learn the signs. Prepare the meds. Train your circle. In a crisis, seconds matter. Be ready.
What is the difference between hypoglycemia and hyperglycemia?
Hypoglycemia is low blood sugar, typically below 70 mg/dL, causing symptoms like shaking and sweating. Hyperglycemia is high blood sugar, usually above 180 mg/dL, leading to thirst, frequent urination, and potentially DKA. They require opposite treatments.
How do I know if someone needs glucagon?
If the person is unconscious, seizing, or unable to swallow safely, they need glucagon. Do not attempt to feed them orally. Administer glucagon via nasal spray or injection and call emergency services immediately.
Can hyperglycemia be treated at home?
Mild hyperglycemia can be managed with extra insulin and water. However, if blood sugar exceeds 250 mg/dL with positive ketones, or if the person is vomiting or confused, seek emergency hospital care. DKA and HHS require IV fluids and insulin.
Which glucagon is better: nasal or injectable?
Nasal glucagon (Baqsimi) is easier to use and has higher success rates among untrained users. Injectable autoinjectors (Gvoke) are effective but require needle handling. Both are superior to traditional mix-and-inject kits for emergency situations.
What are the symptoms of Diabetic Ketoacidosis (DKA)?
Symptoms include high blood sugar, frequent urination, extreme thirst, nausea, vomiting, abdominal pain, fruity breath odor, and rapid, deep breathing. It is a medical emergency requiring immediate hospital treatment.






Write a comment