


Imagine waking up with a sharp, electric shock running from your neck down to your fingertips, or a searing pain that shoots from your lower back all the way to your big toe. This isn't just a "sore muscle" or a simple ache; it's the feeling of a nerve being pinched in your spine. Whether it's in your neck or your lower back, this condition is called radiculopathy. The good news? About 85% of people get better with conservative treatment within three months. You don't always need surgery to get your life back, but you do need a plan that actually targets the specific nerve that's acting up.
What Exactly is Radiculopathy?
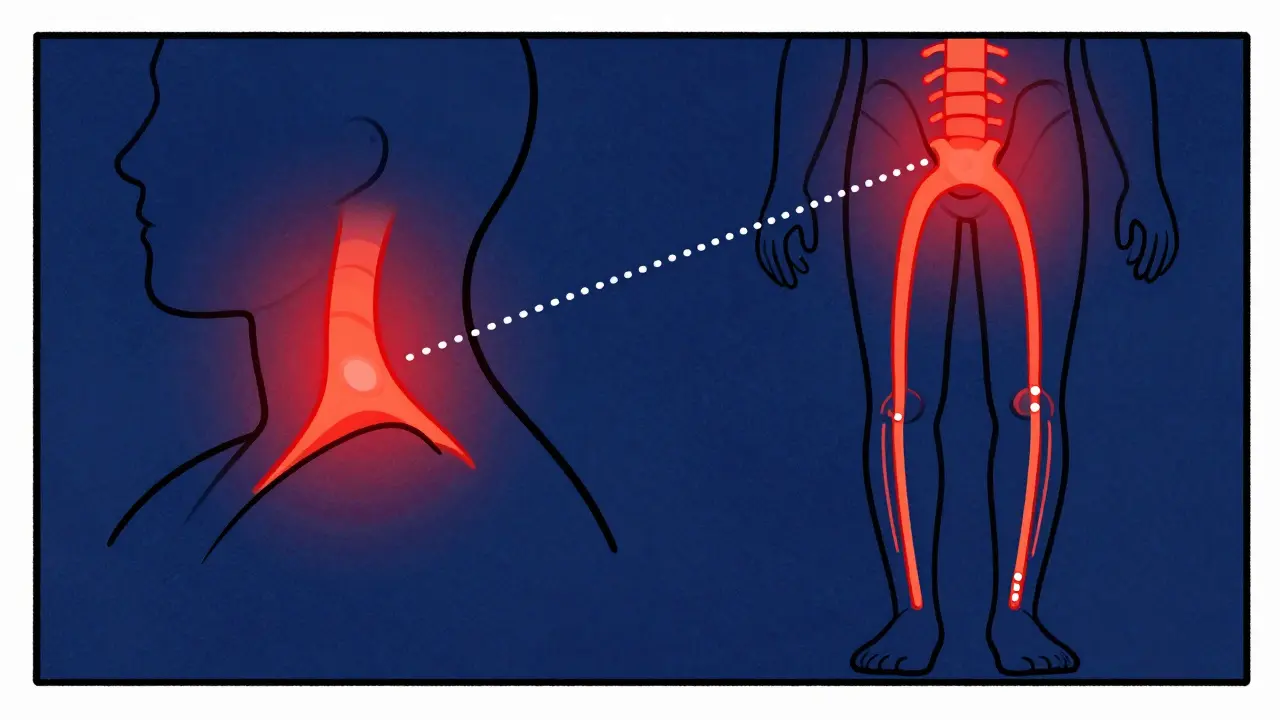
In simple terms, Radiculopathy is a neurological condition where a nerve root in the spinal column becomes compressed or irritated. Think of your spinal nerves like electrical wires. When a disc slips or bone spurs grow, they "pinch" the wire. This interrupts the signal, leading to pain, numbness, or weakness in the area that the specific nerve controls.
Depending on where the pinch happens, you'll feel it in different places. If it's in your neck, it's Cervical Radiculopathy. If it's in your lower back, it's Lumbar Radiculopathy (which many people know as sciatica). While they feel different, the root cause is usually the same: something is pressing on a nerve root as it exits the spine.
Cervical vs. Lumbar: Where is the Pain Coming From?
Not all nerve pain is created equal. Your body follows a map called dermatomes-specific areas of skin served by a single spinal nerve. If you know where the pain is, you can usually guess which nerve is the culprit.
In the neck, the C7 nerve is the most common offender, affecting about 57% of cases. If you feel pain in your middle finger or weakness when straightening your arm (triceps), that's likely the C7. C6 usually hits the thumb and index finger. In the lower back, it's a different story. L5 and S1 are the heavy hitters here. L5 pain typically travels down the outer calf to the big toe, often causing a "foot drop" where you struggle to lift the front of your foot.
| Feature | Cervical (Neck) | Lumbar (Lower Back) |
|---|---|---|
| Commonly Affected Nerves | C6, C7 | L5, S1 |
| Primary Symptoms | Arm pain, finger numbness, grip weakness | Leg pain, calf numbness, ankle weakness |
| Main Cause (< 50 years) | Herniated Disc (90%) | Herniated Disc (90%) |
| Main Cause (> 50 years) | Spondylosis / Stenosis (78%) | Degenerative changes / Stenosis |
| Avg. Recovery Time | ~11 weeks | ~14 weeks |
Why Did This Happen?
If you're under 50, the most likely culprit is a Herniated Disc. This happens when the soft center of a spinal disc pushes through a crack in the tougher exterior, pressing directly on the nerve. If you're over 50, it's more likely due to Spondylosis-essentially wear and tear. Over time, the spaces where nerves exit the spine (the foramina) narrow, a condition called stenosis.
Your job and habits play a huge role too. People in construction or healthcare are over three times more likely to deal with this than the average person. Lumbar issues are strongly linked to heavy lifting, while cervical issues are more often tied to acute trauma or the "tech neck" caused by staring at screens for hours.
The Path to Recovery: Rehab and Management
You might be tempted to jump straight to a surgeon, but hold on. Experts suggest that 90% of neck cases and a huge chunk of back cases improve with nonsurgical therapy. The key is to move through a structured progression rather than doing random stretches you found online.
For those dealing with cervical radiculopathy, the journey usually looks like this:
- Phase 1 (Weeks 2-4): Focus on reducing inflammation with NSAIDs (like ibuprofen) and using gentle cervical traction to create space for the nerve.
- Phase 2 (Weeks 4-8): Introducing isometric strengthening-where you contract the muscle without moving the joint.
- Phase 3 (Weeks 8-12): Dynamic stabilization and ergonomic changes to your workstation.
For lumbar issues, the approach shifts. Instead of just "stretching the hamstring," most successful rehab focuses on McKenzie extension exercises and core stabilization. These movements help "centralize" the pain, moving it from your leg back into your lower back, which is a sign of healing.

Pitfalls and Pro Tips for Faster Healing
Why do some people recover in 8 weeks while others struggle for a year? It usually comes down to consistency and caution. A huge mistake is returning to heavy lifting too early, which causes a symptom recurrence in nearly 30% of patients. Another common trap is "cookie-cutter" physical therapy. If your therapist gives you the same five exercises they give everyone, you're missing out. Personalized programs-those based on exactly which nerve root is pinched-have a much higher completion and satisfaction rate.
If you work in an office, don't ignore your setup. Simple ergonomic modifications can reduce symptoms by about 32%. Use a monitor riser so you aren't tilting your head down, and consider a lumbar support chair that maintains the natural curve of your spine.
When is it an Emergency?
While most cases are manageable, there are a few "red flags" that mean you need to stop reading this and go to the ER. If you experience a sudden loss of bowel or bladder control, or if you have "saddle anesthesia" (numbness in the groin area), you might have Cauda Equina Syndrome. This is a surgical emergency. Similarly, if you notice rapidly progressing muscle weakness (like your foot suddenly dragging on the floor), get a surgical consultation immediately.
Do I really need an MRI to diagnose radiculopathy?
Not always for the initial diagnosis, but it's the gold standard for precision. MRIs have about 92% sensitivity for detecting cervical disc herniations. If conservative treatment isn't working after 6-8 weeks, an MRI helps your doctor see exactly where the compression is happening to plan the next move.
Are epidural steroid injections worth it?
It's a mixed bag. Some patients find them life-changing, but clinical data from the Cochrane Database suggests they mostly provide moderate short-term relief (2-6 weeks) without long-term benefits. They are best used as a "bridge" to get you through the worst pain so you can actually participate in physical therapy.
Can I fix this with just a better pillow?
A pillow won't cure a herniated disc, but it prevents the problem from getting worse. For cervical radiculopathy, proper support keeps the neck in a neutral position, preventing further nerve irritation during the 8 hours you spend sleeping.
How long does the pain usually last?
Most people see significant improvement within 12 weeks of conservative care. However, recovery for lumbar cases tends to be about 28% longer than for cervical cases. Long-term data shows that about 82% of patients return to their full pre-symptom function within a year.
What is the difference between radiculopathy and a pinched nerve?
In common conversation, they are the same thing. "Pinched nerve" is the layperson's term, while "radiculopathy" is the clinical term used by doctors to describe the injury or dysfunction of the nerve root as it leaves the spinal cord.



















Robin Walton
11 Apr 2026 at 05:08Dealing with this kind of pain is honestly exhausting, so it's really encouraging to see that most people recover with just conservative treatment. It makes the whole process feel a bit less daunting for those of us currently in the thick of it.